



Skin Punch Biopsy - Bisected
Picture shows a bisected (cut in half) skin punch biopsy. The skin surface (epidermis) is at the bottom, the white layer is the dermis, and the yellow part is the subcutaneous fat (deepest layer of the skin). The punch biopsy is in a "cassette" (a small rectangular cage) which is sealed with a lid, then immersed in 10% formalin for fixation. The flat surface on the front of the cassette is where the patient identifiers are permanently etched.


Embedding the tissue pieces
Skin tissue after processing. The tissue is taken out of the cassette and placed into a mould with melted paraffin wax. It's cooled slightly, and the cassette with the patient details is placed on top. Then it's sat on ice, which solidifies the whole thing.

Paraffin block after embedding
This image shows how the tissue has the wax in and round it, which makes the next stage possible - cutting paper thin sections on a microtome. Note: this tissue has already been cut into, so you can see the 'full face' of the tissue pieces.

Block in the microtome
A tissue block in the microtome vice. A wheel makes the block go up and down against the blade, allowing very thin sections to be cut from the tissue.

Cutting a "ribbon"
The cutting motion makes a "ribbon" of adjoining sections. You take a length of ribbon and float on the waterbath, to assess quality before picking up on a slide.

Floating the tissue
Now the tissue is floated on the waterbath it can be picked up on a slide, dried out, and is ready for staining. The tissue in this section is from the appendix.

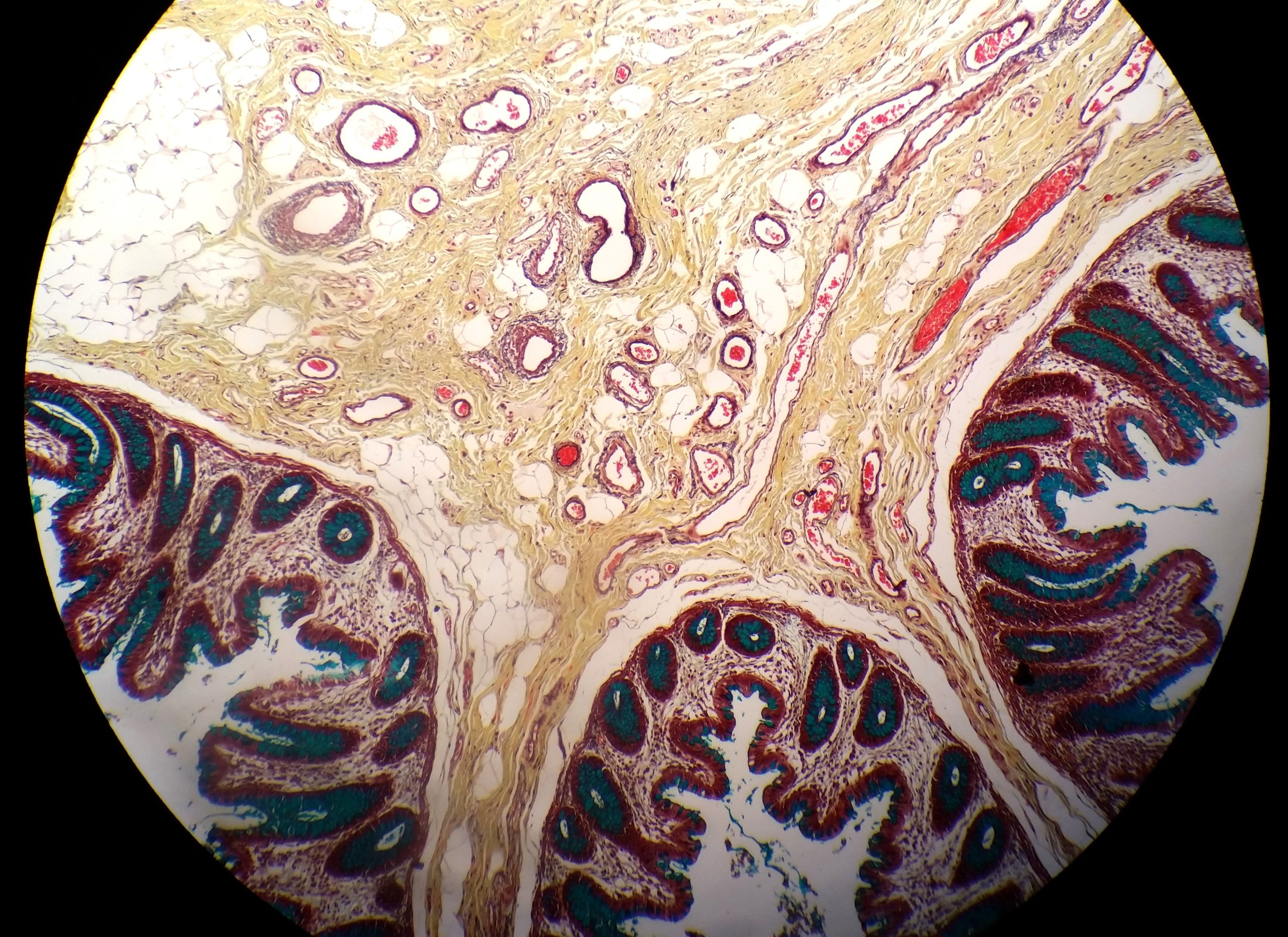
Section of bowel tissue
H&E stained section of bowel (intestine). Note the dark and light areas; haematoxylin is deep pink/purple, while the eosin is light pink, showing different cellular features.

Section of brain tissue
Brain tissue stained with H&E shows
the difference between the "white matter" and "grey matter" areas
within the brain.

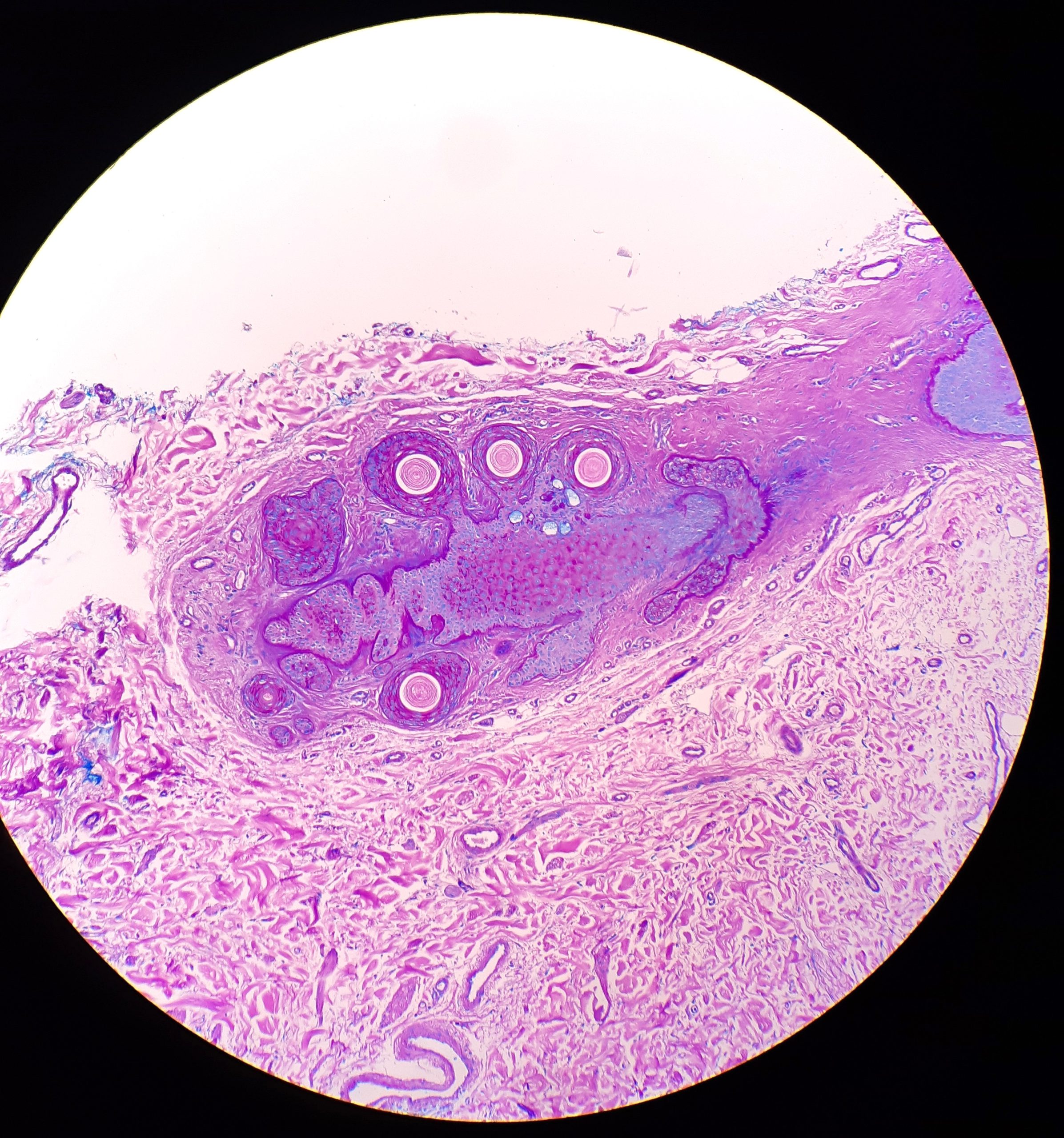
Section of skin tissue
This H&E stained slide shows skin
tissue. It was sliced like a loaf of
bread and laid on its side to get a
full-thickness view through all layers.

{kind=link}
{kind=link}
{kind=link}